
By Howard J. Dananberg, DPM
As described in previous articles in this series, chronic lower back pain (CLBP) can have its origin within the gait cycle and lower extremity (LE) function in particular. Considering that individuals will take between 5-10,000 steps/side/day on average, having dysfunction within the lower extremity can produce a repetitive strain injury (RSI) on par with any other repetitious activity known to cause symptoms. While impact shock has been theorized as the traumatic event during gait, other factors may be far more important when considering how the lumbar spine can be stressed during walking.1
There are three basic factors present during the various phases of any step that can be repetitively stressful to the lower back. These including flexion of the lumbar spine during mid single support phase and iliopsoas activity and lateral trunk bending at toe off. While each of these mechanical dysfunctions can exist as individual entities, it is best to view the events present during walking as a continuum, with one aspect either leading to or perpetuating the other(s).2
During the earlier articles of this series, the mechanics of swing phase was described as the “pull” to create the power for any step.3 For this to occur normally, as the swing limb extends in front of the body, the trailing (weight bearing) limb moves rearward into its maximum extended position. Extension of the trailing limb occurs during single support phase, and terminates immediately with the onset of double support phase.
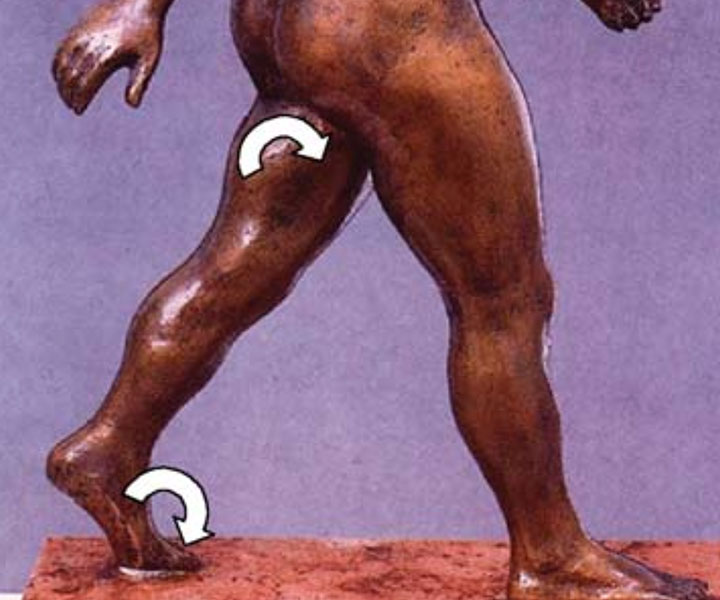
As single support transitions into double support, the trailing limb reverses from extension to flexion, accelerating rapidly until toe off. Just like rearing back to throw a ball, the ability to extend the limb during single support produces a “pre-load” position, storing potential energy to be later returned as kinetic energy during the “pre- swing” phase of gait. With proper extension, the power burst supplied by the iliopsoas (hip flexors) will act on a limb already in motion. Considering that an average hip, thigh and lower leg/foot weigh 15% of body weight, this efficiency is essential to prevent muscular overuse and tissue strain.4
The concept of sagittal plane restriction has been the basis of this series of articles. For the LE to extend normally over the weight bearing foot, the weight bearing foot must permit this motion to occur above it. Failure of this sagittal plane pivot can therefore prevent normal extension at the hip joint, and it often replaced by a subtle but repeatable flexion of the torso. It is these two, mechanically linked processes, which form the basis of understanding how gait mechanics and lower back pain are linked.5
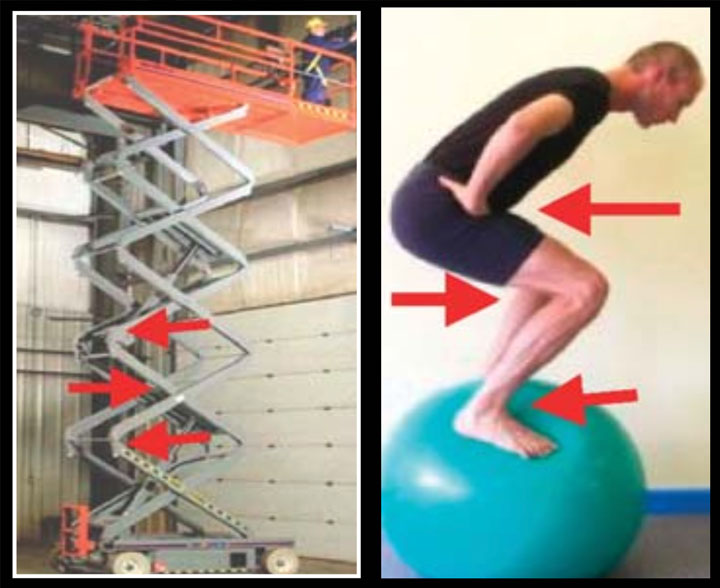
Motions of the hip, knee, and ankle/MTP joints act in the opposite direction from the one directly above or below it. For example, when an individual squats, the ankle and hip flex in the reverse direction of the knee. This is analogous to the motions of a scissor jack. Each of the hinges flex in opposite direction to one another. Should one of these hinges be fused, then motion within the entire jack will cease. This is because these motions are interdependent. Considering that the linkage of the LE is identical to the scissor jack, then loss of motion in one joint will have to negatively impact the others.
The gait style of subjects with osteo-arthritis of the hip joint is well known. They have a characteristic method in which the loss of hip extension is accommodated with knee and ankle flexion. Since the hip joint and foot produce same sagittally directed motion at precisely the same time within the cycle, then loss of foot pivot can produce an effect consistent with loss of hip motion. Herein lies the conundrum. Any failure to produce extension of the weight bearing limb during single support phase will result in a failure to pre-load the limb for the ensuing swing phase.
The iliopsoas takes its origin from the lumbar spine, its disks, vertebra and innerosseous septa. During the time of psoas firing, the vertebra column should normally be extended into lordosis. This permits the facets to articulate in a manner that restricts rotation of the lumbar column. Since the intervertebral disks are very strong to vertical load, yet weak to rotational or axial loading, this stabilization effect becomes essential in maintaining a healthy lumbar spine. Failing to stabilize against rotation, particularly at the time the iliopsoas is firing, produces an environment that is unable to guard against the repetitive stress of thousands of swing phase initiations that occur on a daily basis.
When the foot fails to provide normal pivotal mechanics, lower extremity extension is limited and adjusted for by flexion of the torso. Failing to extend the thigh from beneath the hip, results in a loss of pre-load mechanics. The weight bearing limb is for all intents and purposes “stuck”, and the body is now assigned the task of “dragging” this limb into motion. It is this overall process that can either cause or perpetuate a state of lower back pain.6

One common solution for “dragging” this limb into motion is the lateral trunk bend. This occurs away from the restricted side. For instance, if the right limb’s extension is restricted, it is the left side of the body that must assist in swing phase initiation. For this purpose, the contralateral quatratus lumborum and gluteals through the iliotibial band will fire out of phase to produce a lateral trunk bend. This is so common as to appear as a reflexive motion within the population. Considering that the quadratus lumborum has a substantial insertion to the iliolumbar ligament, it now can affect a rotational moment to the L5 vertebra. Should flexion accommodation of the lumbar spine be present, then there is no osseous guarding available. It would appear as no wonder that 95% of all lumbar disk herniation be L4-5 and L5-S1 considering the above.
In order to address these issues, careful biomechanical evaluation of the lower extremity is essential. Motion of the pivotal segments of the ankle and MTP joint must be assessed so as to determine the impact any restriction may have on lower back mechanics. Should Fhl be detected, then, appropriate modification of foot orthoses is critical to re-establish proper MTP joint mechanics. This is the entire purpose of the Vasyli-Dananberg orthotic device. By utilizing a multi stage removable plug on the plantar surface of the 1st metatarsal head, adequate plantarflexion can be restored and Fhl and its sequealae prevented.

The device is designed so that different levels of functional locking can be addressed, but simply removing additional material from under the device. Care should also be taken to address any leg length difference that may exist, and heel lifts are available for this very purpose.
Conclusion
Previous studies have shown that 84% of patients considered at or near medical endpoint for chronic lower back pain can have major improvements in symptoms via the foot orthotic approach. Care in assessment and proper orthotic prescribing is essential to achieve this very positive outcome.

REFERENCES:
1. Dananberg HJ. Gait style as an etiology to chronic postural pain, part II The postural compensatory process. J Am Podiatr Med Assoc 1993; 83(11):615- 624
2. Dananberg, HJ. Lower back pain as a gait related repetitive motion injury. In: Vleeming A, Mooney V, Dorman T, et al, eds. Movement, stability and lower back pain. Edinburgh: Churchill Livingstone 1997: page 253.
3. Claeys, R.,1983, The Analysis of Ground Reaction Forces in Pathologic Gait, International Orthopaedics, Spring 113-119
4. Dananberg, H J, 1995 Lower Extremity Mechanics and Their Effect of Lumbosacral Function, Spine, State of the Art Reviews, Ed. Dorman, T, Henley & Belfus, Philadelphia May 9:2 389-405
5. Dananberg, HJ, “Gait Style and Its Relevance in the Management of Chronic Lower Back Pain”, In Proceedings, 4th Interdisciplinary World Congress of Low Back & Pelvic Pain”, Ed, Vleeming, A, Mooney. V, Gracovetsky, S, Lee, D, etal, November 8-10, 2001, pp 225-230
6. Dananberg, HJ, Guiliano, M, “Gait Mechanics and Their Relationship to Lower Back Pain”, in Proceeding of 3rd Interdisciplinary World Congress on Low Back and Pelvic Pain, Vleeming, A, Mooney, V, Tilscher, H, Dorman, T, and Snijders, C, November, 1998, European Conference Organizers, Rotterdam, Holland
7. Dananberg, HJ, Guiliano, M, “Chronic Lower Back Pain And It Response to Custom Foot Orthoses”, Journal of the American Podiatric Medical Association, 89:3 March, 1999 pp109-117